











Editorial: Unethical data reporting behind 2nd wave hysteria
Of great concern is the apparently questionable data used as the foundation of the 2nd wave analysis. Unless the AUH has access to a time machine, reporting future projections as actual data is not only unprofessional, but also unethical.

Facts, not hysteria, will defeat a 2nd wave
Fearful of a significantly higher case number over the past 3 weeks, the Lebanese government has reimposed restrictions for a 2-week period, including a 4-day lockdown to limit so-called “super spreader” events around Eid al-Adha. There is also a renewed push to wear masks in public places and respect social distancing guidelines. While citizens have a duty to comply in order to inhibit the spread of the virus, responsibility goes both ways.
The government’s current decision may befit the circumstances, but imposing draconian restrictions that impact lifestyles - and especially economic well-being - can no longer be justified without a robust explanation. Hysteria as a means of scaring people into changing behavior may have seemed normal in March, but it is not sustainable today.
For example, consider the information communicated by Petra Khoury, Chief Quality and Compliance Officer of the American University Hospital, who also serves as Prime Minister Hassan Diab’s key advisor for COVID-19. Last weekend, she tweeted a series of 4 graphs illustrating the dramatic case increase. Accompanying these visuals was the text “We will soon start seeing horrific images in our hospitals like other countries. At this pace, critical care beds will fill by mid-August. We are at a very dangerous point!”
To the casual observer, Dr. Khoury’s authority alone would suffice to accept her argument. But a more critical look reveals numerical errors, misleading data, incomplete logic and doubtful conclusions, all of which make the inflammatory statement about “horrific images” even more inappropriate and unhelpful.

Dr. Khoury cited on July 24 an 80% increase in the case number since “lifting lockdown” on June 8. (It was actually a 150% increase, but that is not really the point.) As her graph shows, the case trend remained linear until about July 8, one month after all restrictive measures had ended. In fact, the lifting of phases 2-5 of lockdown measures during May led to a greater proportional increase of cases than the full lifting. So what changed a whole month later on July 8? Was it the airport? Was it more social gatherings and a festive summer environment? Was it simply increased testing? The simple causation in Dr. Khoury’s graph does not sufficiently explain.
More troubling is her graph regarding ICU patients, on which she claims that critical care capacity (~270 beds) will be reached on August 14 with a 10% growth in cases. Yet she does not specify over what time period this 10% would need to occur. Is it daily? Weekly? Additionally, the same graph’s y axis refers to a 6% growth in cases, not 10%. This is just confusing and poorly explained.

Dr. Khoury cites a 25% growth in ICU cases between July 20 and 24, yet according to the Ministry of Health, ICU cases stood at 15 on July 20 and 21 on July 24. That’s a 40% increase, not 25% - but once again, her math errors are the least of our worries.
Of much more concern is the apparently questionable data used as the foundation of her analysis. Dr. Khoury’s graph dated July 23 seems to show a value of approximately 50 cases at the last recorded data point, which appears to be on July 27 or 28, several days subsequent to her post. Something is obviously wrong, unless the AUH has access to a time machine.
Reporting future projections as actual data is not only unprofessional, but also unethical. (For the record, the ICU case number did in fact peak on July 27, 3 days later than her post, but at 36 patients - not 50.)
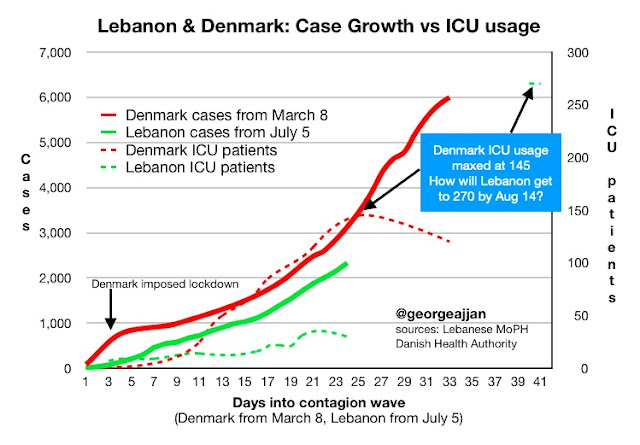
Then there’s the matter of her projection itself. On what basis does she conclude that the expected number of ICU patients will go sharply up in exponential fashion? If we compare Lebanon to Denmark, which has a similar population size and saw a similar explosion of cases during the first wave, we might find her proposed trajectory unlikely and doubt that Lebanon would exceed its ICU capacity. Denmark’s ICU usage peaked at only 145 patients in less than a month.
Still, Dr. Khoury and her colleagues advising the Prime Minister may be right to believe that Lebanon will exceed ICU capacity. That would indeed be horrific. If so, they owe us a more robust explanation so that we can better grasp the risks. Understanding the threat leads to more confidence in the measures and thus greater solidarity so that we can defeat the virus more quickly.
A second wave of COVID-19 could pose great danger. If that is the case, compliance with measures will be essential. But it must be gained with robust logic, not hysteria based upon dubious data reporting.